Norwegian society of rheumatology recommendations on diagnosis and treatment of patients with giant cell arteritis
 Anne Bull Haaversen1
Anne Bull Haaversen1  Lene Kristin Brekke2 Gunnstein Bakland3 Erik Rødevand4 Geirmund Myklebust5 Andreas P. Diamantopoulos6*
Lene Kristin Brekke2 Gunnstein Bakland3 Erik Rødevand4 Geirmund Myklebust5 Andreas P. Diamantopoulos6*- 1Department of Rheumatology, Martina Hansens Hospital, Bærum, Norway
- 2Department of Rheumatology, Hospital for Rheumatic Diseases, Haugesund, Norway
- 3Department of Rheumatology, University Hospital of Northern Norway, Tromsø, Norway
- 4Department of Rheumatology, St. Olav’s University Hospital, Trondheim, Norway
- 5Department of Research, Hospital of Southern Norway, Kristiansand, Norway
- 6Department of Infectious Diseases, Division of Internal Medicine, Akershus University Hospital, Lørenskog, Norway
Objective: To provide clinical guidance to Norwegian Rheumatologists and other clinicians involved in diagnosing and treating patients with giant cell arteritis (GCA).
Methods: The available evidence in the field was reviewed, and the GCA working group wrote draft guidelines. These guidelines were discussed and revised according to standard procedures within the Norwegian Society of Rheumatology. The European Alliance of Associations for Rheumatology (EULAR) recommendations for imaging and treatment in large vessel vasculitis and the British Society for Rheumatology (BSR) guidelines for diagnostics and treatment in GCA informed the development of the current guidelines.
Results: A total of 13 recommendations were developed. Ultrasound is recommended as the primary diagnostic test. In patients with suspected GCA, treatment with high doses of Prednisolone (40–60 mg) should be initiated immediately. For patients with refractory disease or relapse, Methotrexate (MTX) should be used as the first-line adjunctive therapy, followed by tocilizumab (TCZ).
Conclusion: Norwegian recommendations for diagnostics and treatment to improve management and outcome in patients with GCA were developed.
Introduction
Background
Giant cell arteritis (GCA) is the most common systemic vasculitis in adults and has a spectrum of possible presentations (1, 2). The main subsets include isolated cranial arteritis (c-GCA), isolated large vessel vasculitis (LV-GCA), and coexisting cranial and large vessel vasculitis (mixed-GCA) (2). Polymyalgia rheumatica (PMR) and GCA are closely related, and some argue that PMR lies within the spectrum of GCA. However, these conditions may occur simultaneously or independently of each other (3–5).
Giant cell arteritis occurs almost exclusively in people older than 50 years of age, with a peak in onset between 70 and 80 years of age and with a female predominance (6, 7). The majority of epidemiological studies on GCA have investigated European or North American populations, and the highest incidence has been reported in Nordic countries or North-American people of Scandinavian descent (8). Data on GCA occurrence in Africa, Asia, the Middle East, South- and Latin America, and Oceania are sparse and suggest that the condition is less common in non-Caucasians.
The annual incidence rate for GCA in Norway was recently estimated to be 22.5 per 100,000 persons ≥50 years of age (7).
Giant cell arteritis’ etiopathogenesis is not fully understood but is considered to involve a combination of genetic and environmental factors (9). Different compositions of genetic background may contribute to global differences. There is also evidence that lifestyle factors such as body mass index, glucose levels, and smoking may influence the risk of GCA (10–14).
Objectives of the guidelines
These recommendations aim to provide clinical guidance to Rheumatologists and other clinicians involved in diagnosing and treating GCA patients. The guidelines cover individuals older than 50 years of age suspected to have GCA. The guidelines aim to harmonize the diagnostic and treatment procedures across specialists and departments in the Norwegian Healthcare System.
Methods
The Norwegian GCA working group (the members are the authors of these guidelines) developed the recommendations by reviewing the available evidence and writing the draft guidelines. The draft guidelines were discussed and revised according to standard procedures within the Norwegian Society of Rheumatology.
The European Alliance of Associations for Rheumatology (EULAR) recommendations for imaging and treatment in large vessel vasculitis (15, 16) and The British Society for Rheumatology (BSR) guidelines for diagnostics and treatment in GCA (17) served as the basis to the development of current guidelines. As the American College of Rheumatology guidelines recommend the use of Tocilizumab very early in the treatment of GCA patients, which is not refunded by the Norwegian Health Authorities, we chose not to incorporate these guidelines in the Norwegian guidelines (18). Also, the evidence on diagnostics and treatment of GCA published after 2018 was reviewed and included in this work. The PubMed and a combination of the search terms Giant cell arteritis and treatment and/or diagnosis were used. The review of individual studies was restricted to randomized controlled studies or prospective observational studies with >50 participants. The guidelines were proposed, discussed, revised, and accepted by voting/reaching an agreement by the majority of the members of the working group and the professional council (in Norwegian: Fagrådet) of the Norwegian Society of Rheumatology. The method used to obtain consensus was voting among members during meetings of the working group.
The present guidelines are the foundation upon which clinical practice should be based. Guidelines, unlike some types of policies, are not mandatory. Individual patient circumstances may influence clinical decisions, and clinicians should work alongside patients to make care-based shared decisions. Thus, failure to adhere to these guidelines should not necessarily be considered negligent. These guidelines should not be used to limit access to other diagnostic or treatment options.
Results
Diagnosis
Recommendation 1
In patients with suspected GCA, a thorough history should be obtained, including inquiry about polymyalgia symptoms, new-onset headache, tongue- or jaw-claudication, vision disturbances, arm or leg claudication, constitutional symptoms (fatigue, fever, and weight loss). Additionally, a thorough clinical examination and laboratory workup should be performed including heart and lung auscultation, blood pressure in both arms, temperature, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and full blood count (Table 1).
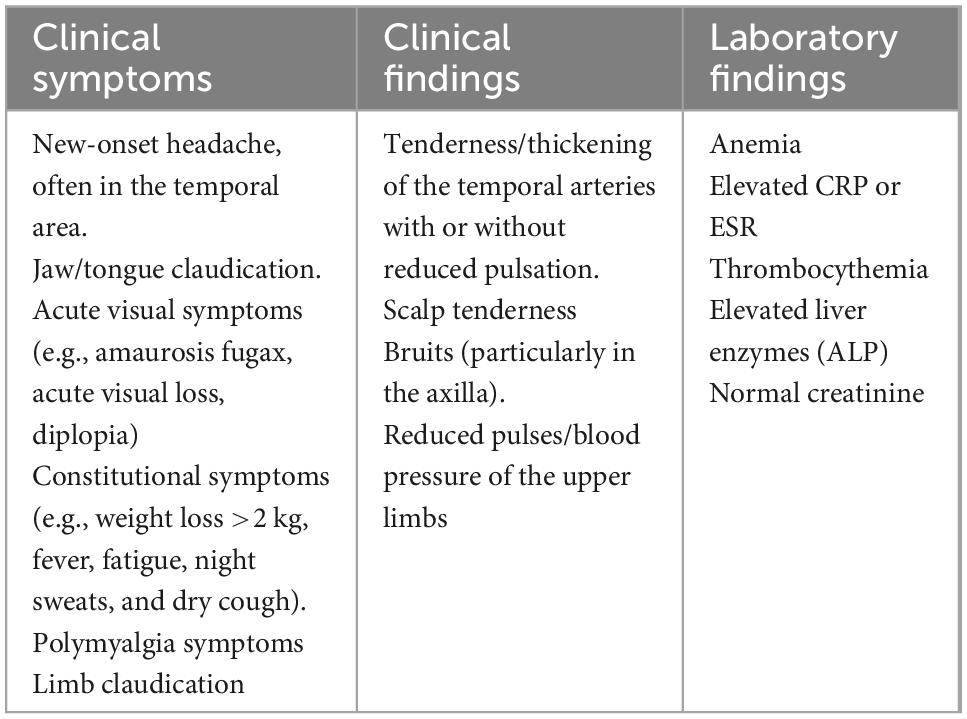
Table 1. Clinical symptoms and findings and laboratory results in giant cell arteritis (GCA) patients.
Recommendation 2
Patients suspected of having GCA, should be directly referred to a Fast-Track Clinic (FTC) or a rheumatologist for further evaluation, treatment, and follow-up within 24 h. In cases where FTC- or rheumatology consult is unavailable within 24 h the patient may be referred to other relevant specialists (e.g., neurologist, ophthalmologist, and internist). FTC consists of an evaluation by ultrasound or other imaging modality which can confirm the diagnosis immediately (19). Diagnostic work-up should not delay the initiation of treatment.
Recommendation 3
In patients with suspected GCA, ultrasound of at least temporal and axillary arteries (20) should be performed by an ultrasonographer experienced in vascular ultrasound using high-end ultrasound equipment (21) (Tables 2, 3). Ultrasound of the facial artery further increases the sensitivity to diagnose GCA (20). If ultrasound is not available or inconclusive, a biopsy of the temporal artery should be considered. The length of the biopsy should be >1 cm after fixation. Giant cells in the biopsy are not obligate for the diagnosis of GCA, but appropriate pathological findings should be present (Table 4). Alternatively, Magnetic Resonance Angiography (MRA) of temporal arteries or Positron Emission Tomography (PET-CT) may be performed. In addition, ultrasound of large vessels (carotid, vertebral, and subclavian) (22) or CT of large vessels or MRA or PET-CT depending on the availability is recommended. It is essential to recognize the disease extent as early as possible as large vessel involvement may indicate difficult-to-treat disease, while temporal artery involvement has been associated with a higher risk for visual loss (23, 24). The choice of imaging modality depends on the local availability.
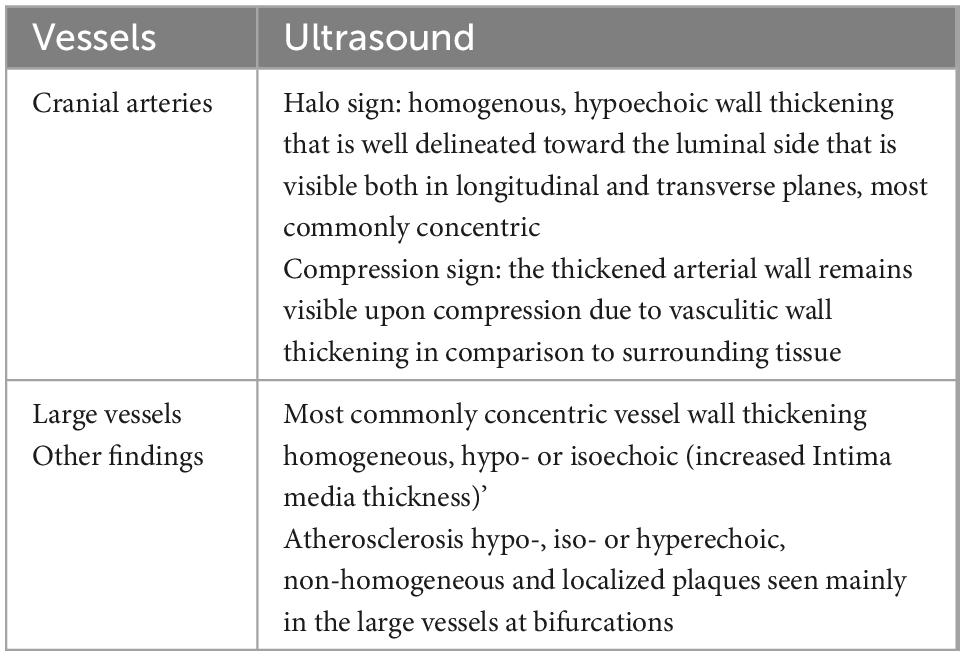
Table 2. Ultrasonographic findings in giant cell arteritis (GCA) patients (33).
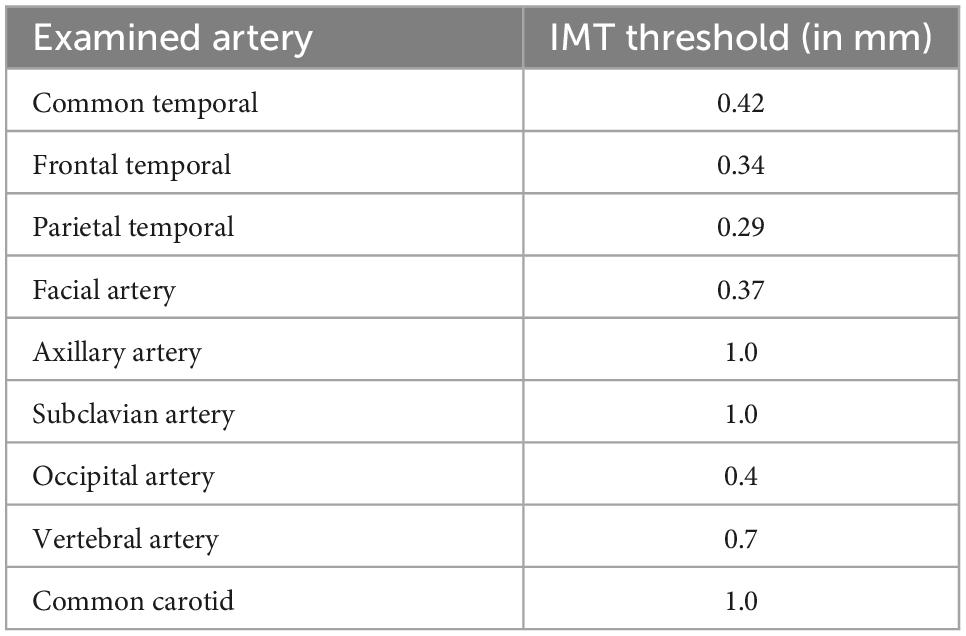
Table 3. Threshold intima media thickness (IMT) values in ultrasound examination (34).
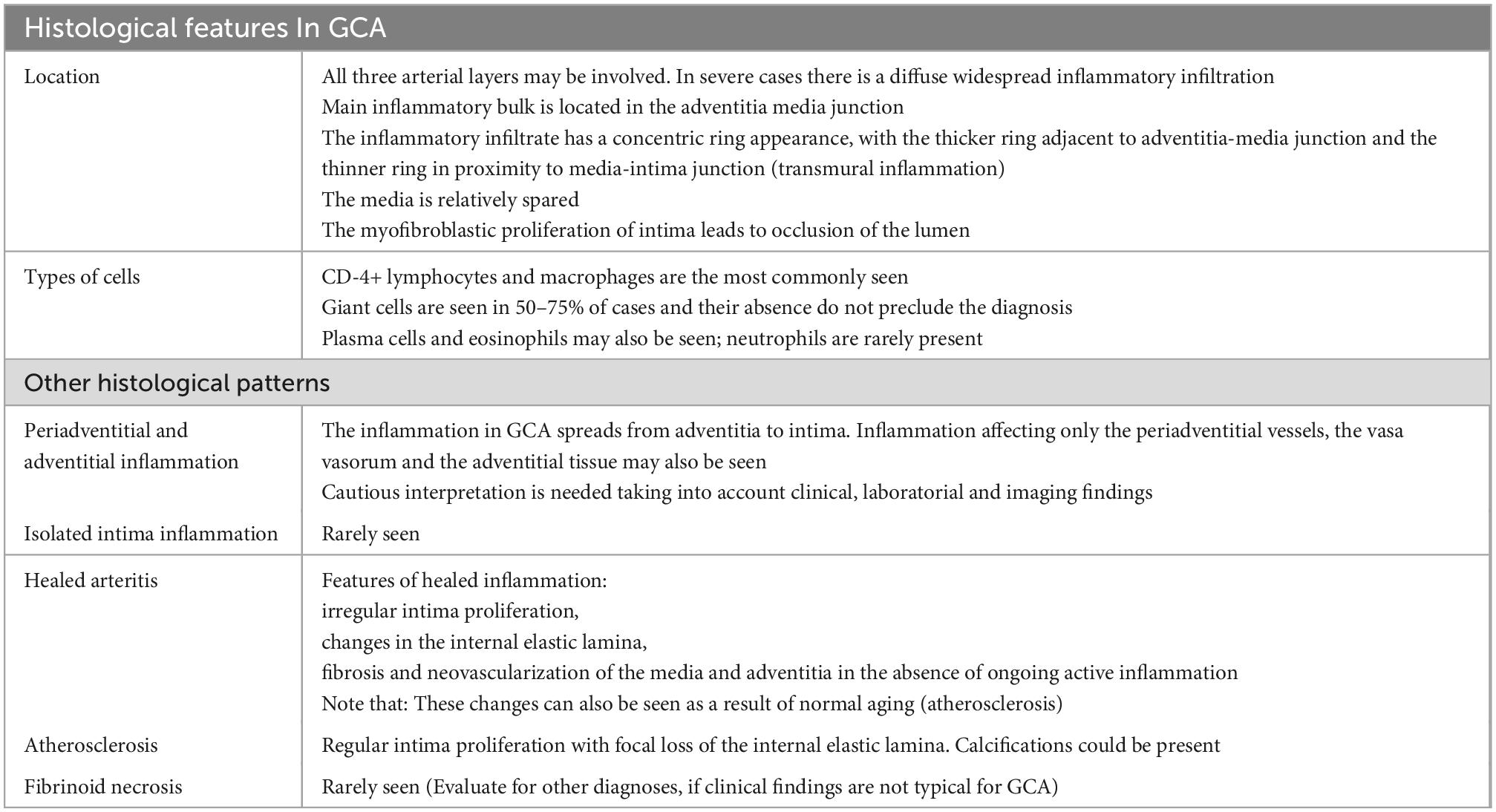
Table 4. Histological findings in patients with giant cell arteritis (GCA) (35).
Recommendation 4
In a patient with high clinical suspicion of GCA and a positive diagnostic test (biopsy or imaging modality), no further test is required to confirm the diagnosis. In patients with low clinical suspicion of GCA and a negative diagnostic test (biopsy or imaging modality), the probability for GCA is low. In other cases, an individual assessment will be necessary for further diagnostics.
Recommendation 5
In patients with GCA and visual symptoms, referral to an ophthalmologist is highly recommended. Initiation of treatment should not be delayed while waiting for this evaluation (Figure 1 and Table 5).
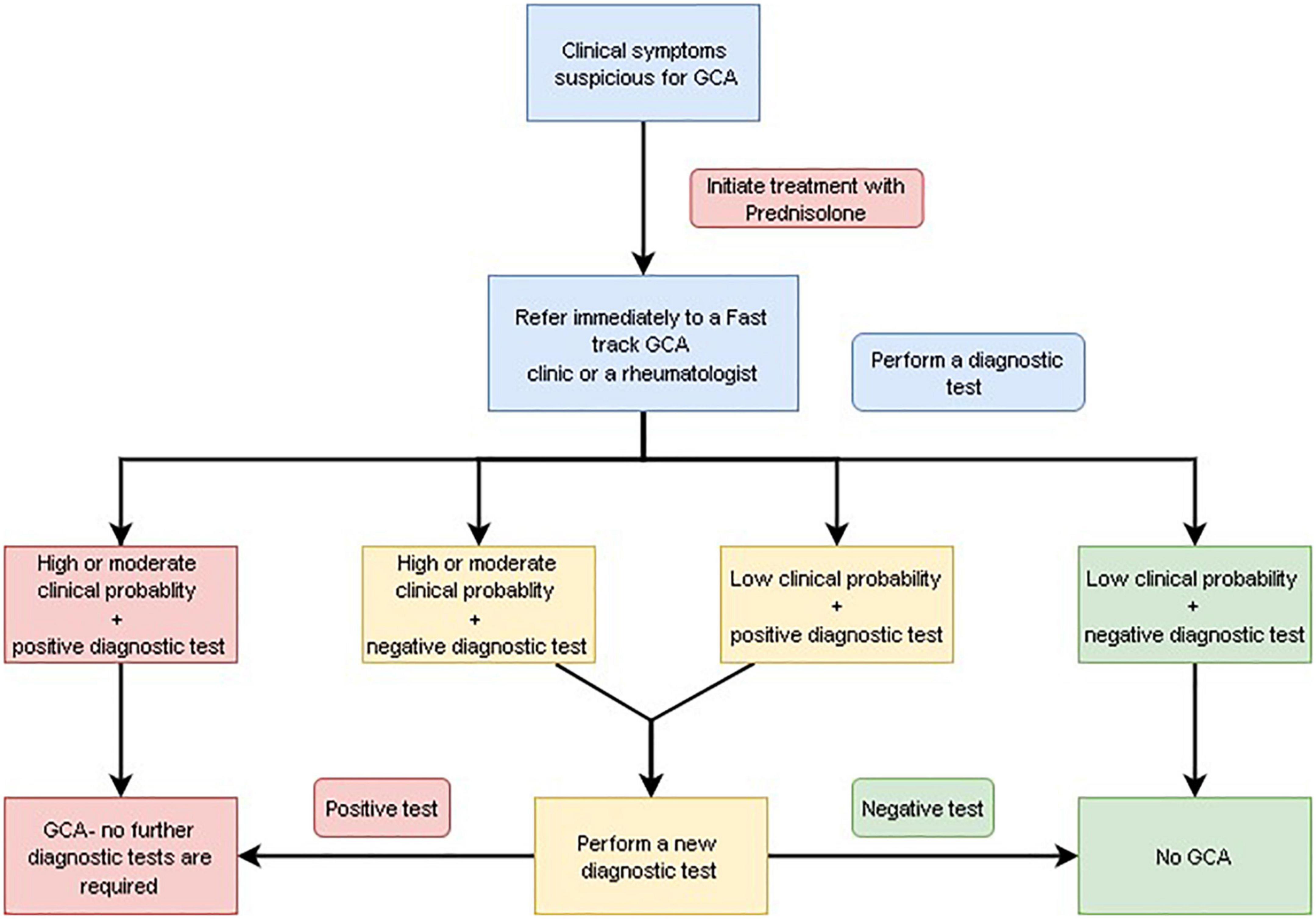
Figure 1. Diagnostic algorithm for giant cell arteritis (GCA).
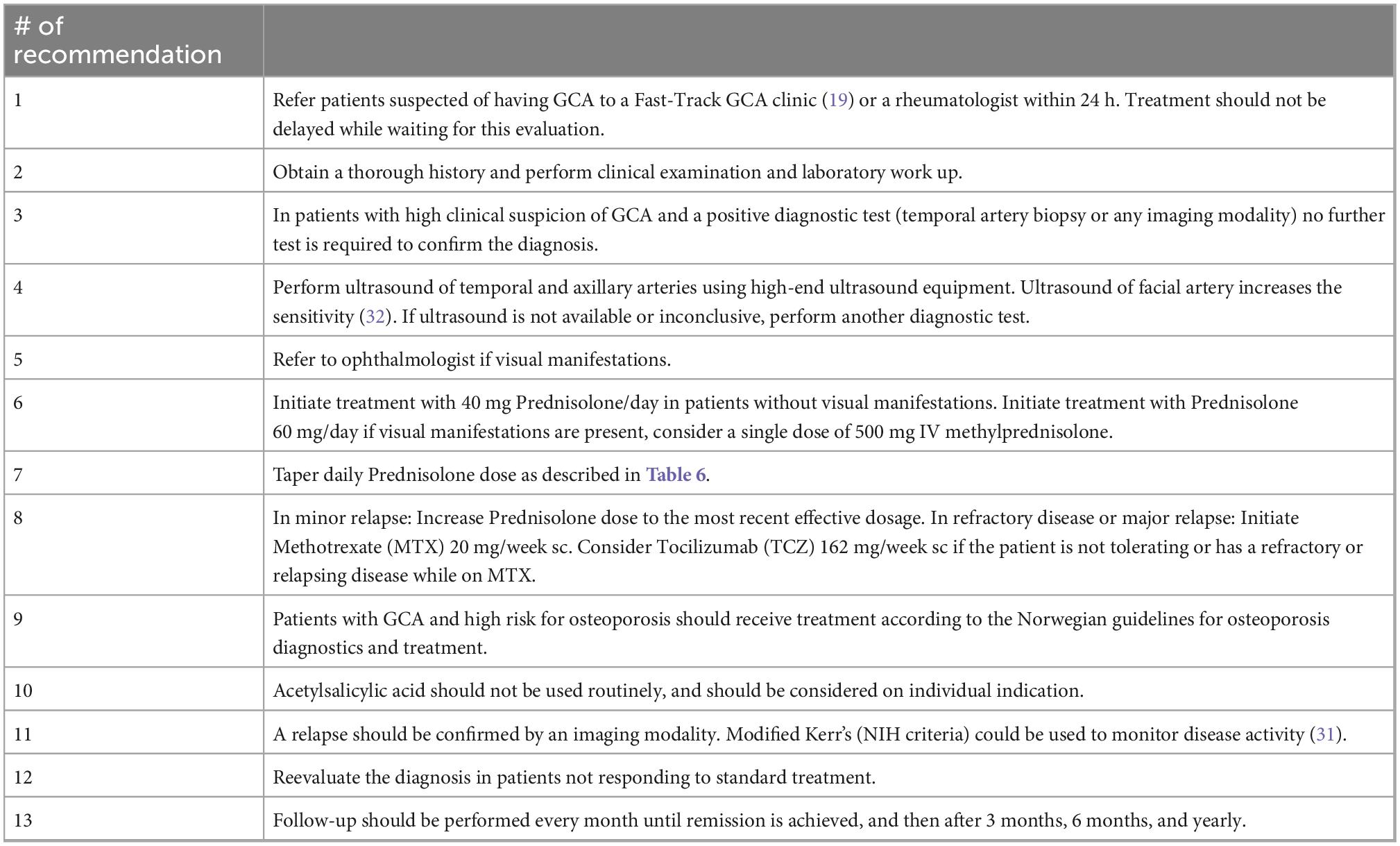
Table 5. Summary of the Norwegian society of rheumatology’s recommendations on diagnosis and treatment of patients with giant cell arteritis (GCA).
Treatment
Recommendation 6
In patients with suspected GCA, glucocorticoids should be immediately initiated. The diagnostic work-up should not delay the initiation of treatment. For patients without visual manifestations we recommend a starting dose of 40 mg Prednisolone/day. In patients with visual involvement (visual loss, diplopia, amaurosis fugax, and blurred vision), we recommend starting with 60 mg Prednisolone/day. A single dose of 500 mg × 1 methylprednisolone iv followed by Prednisolone 60 mg/day may be individually considered, but the evidence is sparse (25–27).
Recommendation 7
In patients with GCA, Prednisolone should be tapered by 5 mg every 2nd week till 20 mg/day, after that with 2.5 mg every 3rd week till 10 mg/day, and after that with 1.25 mg every 3rd week to 5 mg/day. We recommend continuing treatment with 5 mg/day at least for 1 year after initiation of Prednisolone. Further tapering can be considered on an individual basis if the patient has been in remission for at least 1 year. When starting with dose 60 mg/day, Prednisolone should be tapered by 10 mg every week till 40 mg/day, thereafter tapering as described above (Table 6).
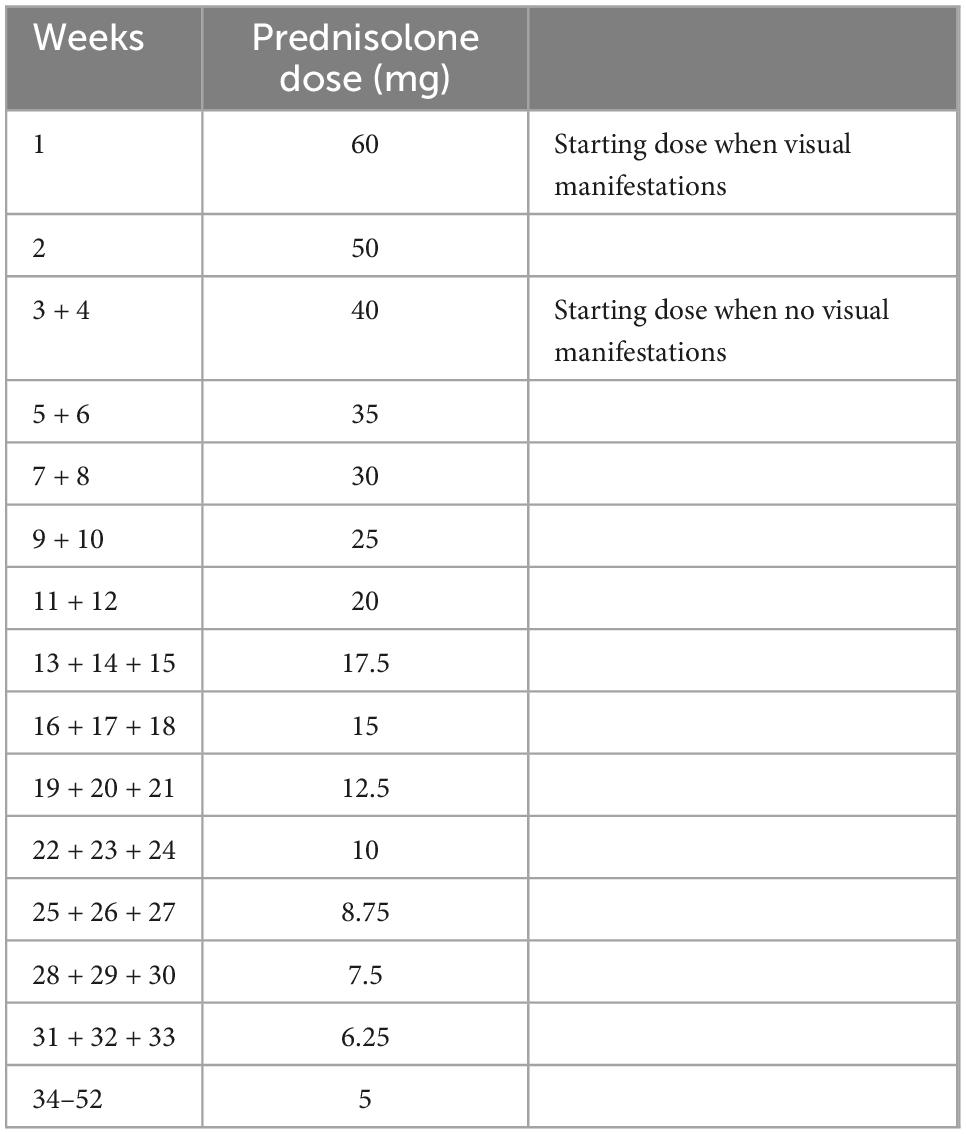
Table 6. Prednisolone tapering.
Recommendation 8
If the patients suffers a relapse, we recommend an increase in Prednisolone dose to the last effective dose, or a higher dose based on the severity of the relapse and an individual assessment. In patients with refractory disease or a major relapse (Table 7), initiation of Methotrexate (MTX), preferably subcutaneously, 20 mg/week, should be considered. The dose should be adjusted according to the patient’s age and kidney function. Tocilizumab (TCZ) 162 mg/week sc should be considered if the patient is not tolerating MTX or suffer a relapse while on MTX (according to the Norwegian Tender System). Leflunomide or Azathioprine may be considered, but evidence supporting their use is scarce. There is currently no robust evidence supporting the use of TNF-α inhibitors or other biologics than TCZ in patients with GCA.
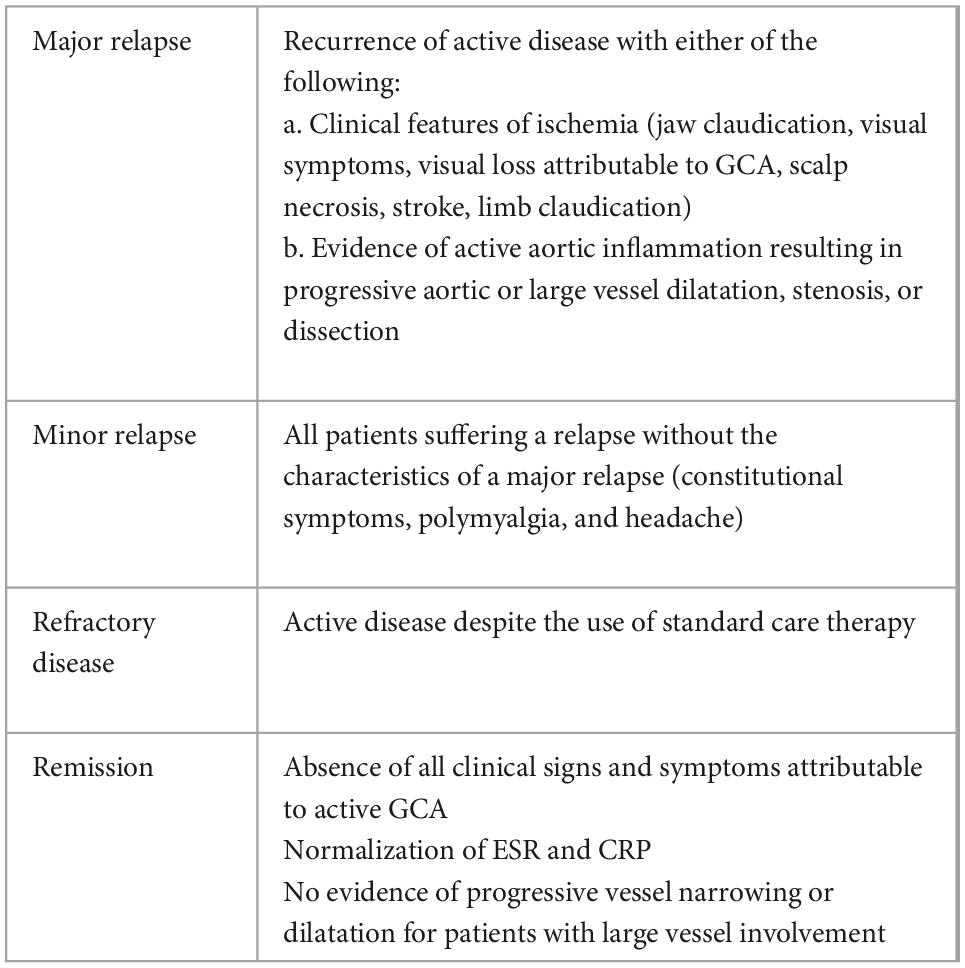
Table 7. Definitions of disease activity (16).
Recommendation 9
Giant cell arteritis patients with new-onset disease should be referred to a measurement of bone mass density. In patients with GCA and high risk for osteoporosis, treatment according to the Norwegian guidelines for osteoporosis should be initiated (28).
Recommendation 10
In patients with GCA, we do not routinely recommend using Acetylsalicylic acid unless cardiovascular reasons support its use (Figure 2).
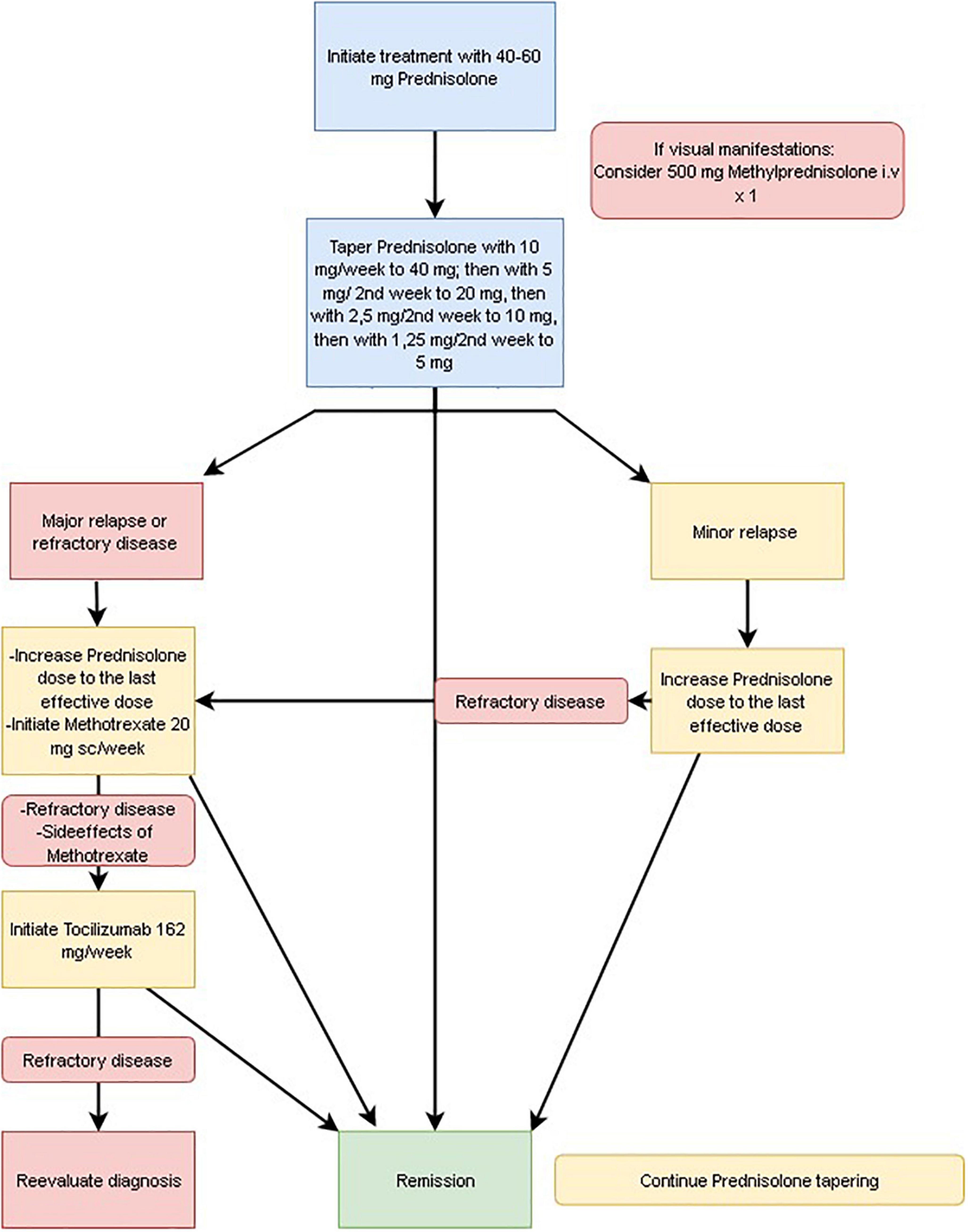
Figure 2. Treatment algorithm for giant cell arteritis (GCA).
Follow up
Recommendation 11
In GCA patients, follow-up should be continued every month until remission is achieved. Thereafter follow-up at 3 months, 6 months, and thereafter yearly.
Recommendation 12
In GCA patients who suffer a relapse, the relapse should, if possible, be confirmed by an imaging modality, preferably ultrasound, and/or laboratory tests (29, 30). Modified Kerr’s (NIH) criteria (originally developed for Takayasu arteritis) may be used to monitor disease activity (31) (Tables 7, 8).
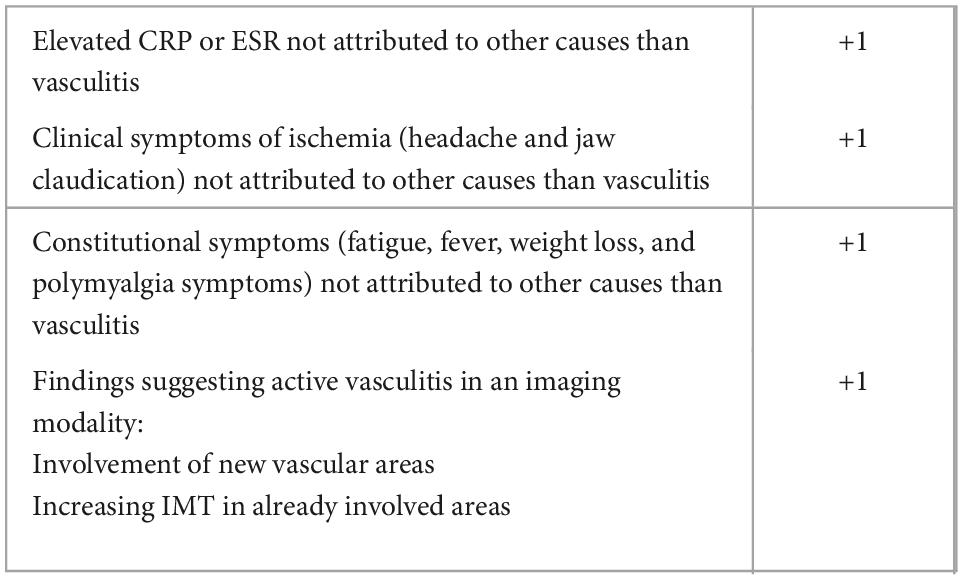
Table 8. Modified Kerr’s criteria: >1 point indicates active disease (31).
Recommendation 13
In GCA patients with relapsing or refractory disease, alternative diagnoses should be considered (e.g., malignancy, autoinflammatory syndromes).
Data availability statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
AH prepared the manuscript. AD, LB, GB, GM, and ER contributed equally to the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Dejaco C, Duftner C, Buttgereit F, Matteson EL, Dasgupta B. The spectrum of giant cell arteritis and polymyalgia rheumatica: revisiting the concept of the disease. Rheumatology. (2017) 56:506–15. doi: 10.1093/rheumatology/kew273
3. Weyand CM, Goronzy JJ. Clinical practice. Giant-cell arteritis and polymyalgia rheumatica. N Engl J Med. (2014) 371:50–7.
4. Schmidt J, Warrington KJ. Polymyalgia rheumatica and giant cell arteritis in older patients: diagnosis and pharmacological management. Drugs Aging. (2011) 28:651–66.
5. Cantini F, Niccoli L, Storri L, Nannini C, Olivieri I, Padula A, et al. Are polymyalgia rheumatica and giant cell arteritis the same disease? Semin Arthritis Rheum. (2004) 33:294–301.
6. Myklebust G, Gran JT. A prospective study of 287 patients with polymyalgia rheumatica and temporal arteritis: clinical and laboratory manifestations at onset of disease and at the time of diagnosis. Br J Rheumatol. (1996) 35:1161–8. doi: 10.1093/rheumatology/35.11.1161
7. Brekke LK, Diamantopoulos AP, Fevang BT, Abetamus J, Espero E, Gjesdal CG. Incidence of giant cell arteritis in Western Norway 1972-2012: a retrospective cohort study. Arthritis Res Ther. (2017) 19:278.
8. Sharma A, Mohammad AJ, Turesson C. Incidence and prevalence of giant cell arteritis and polymyalgia rheumatica: a systematic literature review. Semin Arthritis Rheum. (2020) 50:1040–8. doi: 10.1016/j.semarthrit.2020.07.005
9. Weyand CM, Goronzy JJ. Immune mechanisms in medium and large-vessel vasculitis. Nat Rev Rheumatol. (2013) 9:731–40. doi: 10.1038/nrrheum.2013.161
10. Tomasson G, Bjornsson J, Zhang Y, Gudnason V, Merkel PA. Cardiovascular risk factors and incident giant cell arteritis: a population-based cohort study. Scand J Rheumatol. (2019) 48:213–7. doi: 10.1080/03009742.2018.1506821
11. Ungprasert P, Thongprayoon C, Warrington KJ. Lower body mass index is associated with a higher risk of giant cell arteritis: a systematic review and meta-analysis. Ann Transl Med. (2015) 3:232. doi: 10.3978/j.issn.2305-5839.2015.09.31
12. Jakobsson K, Jacobsson L, Warrington K, Matteson EL, Liang K, Melander O, et al. Body mass index and the risk of giant cell arteritis: results from a prospective study. Rheumatology. (2015) 54:433–40. doi: 10.1093/rheumatology/keu331
13. Brennan DN, Ungprasert P, Warrington KJ, Koster MJ. Smoking as a risk factor for giant cell arteritis: a systematic review and meta-analysis. Semin Arthritis Rheum. (2018) 48:529–37. doi: 10.1016/j.semarthrit.2018.07.001
14. Wadstrom K, Jacobsson L, Mohammad AJ, Warrington KJ, Matteson EL, Turesson C. Negative associations for fasting blood glucose, cholesterol and triglyceride levels with the development of giant cell arteritis. Rheumatology. (2020) 59:3229–36. doi: 10.1093/rheumatology/keaa080
15. Dejaco C, Ramiro S, Duftner C, Besson FL, Bley TA, Blockmans D, et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice. Ann Rheum Dis. (2018) 77:636–43. doi: 10.1136/annrheumdis-2017-212649
16. Hellmich B, Agueda A, Monti S, Buttgereit F, de Boysson H, Brouwer E, et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. (2020) 79:19–30.
17. Mackie SL, Dejaco C, Appenzeller S, Camellino D, Duftner C, Gonzalez-Chiappe S, et al. British Society for Rheumatology guideline on diagnosis and treatment of giant cell arteritis. Rheumatology. (2020) 59:E1–23.
18. Maz M, Chung SA, Abril A, Langford CA, Gorelik M, Guyatt G, et al. 2021 American college of rheumatology/vasculitis foundation guideline for the management of giant cell arteritis and takayasu arteritis. Arthritis Care Res. (2021) 73:1071–87. doi: 10.1002/acr.24632
19. Diamantopoulos AP, Haugeberg G, Lindland A, Myklebust G. The fast-track ultrasound clinic for early diagnosis of giant cell arteritis significantly reduces permanent visual impairment: towards a more effective strategy to improve clinical outcome in giant cell arteritis? Rheumatology. (2015) 55:66–70. doi: 10.1093/rheumatology/kev289
20. Jese R, Rotar Z, Tomsic M, Hocevar A. The cut-off values for the intima-media complex thickness assessed by colour Doppler sonography in seven cranial and aortic arch arteries. Rheumatology. (2021) 60:1346–52. doi: 10.1093/rheumatology/keaa578
21. Chrysidis S, Terslev L, Christensen R, Fredberg U, Larsen K, Lorenzen T, et al. Vascular ultrasound for the diagnosis of giant cell arteritis: a reliability and agreement study based on a standardised training programme. RMD Open. (2020) 6:e001337. doi: 10.1136/rmdopen-2020-001337
22. Bull Haaversen AC, Brekke LK, Kermani TA, Molberg O, Diamantopoulos AP. Extended ultrasound examination identifies more large vessel involvement in patients with giant cell arteritis. Rheumatology. (2022) [Online ahead of print]. doi: 10.1093/rheumatology/keac478
23. Hocevar A, Rotar Z, Jese R, Semrl SS, Pizem J, Hawlina M, et al. Do early diagnosis and glucocorticoid treatment decrease the risk of permanent visual loss and early relapses in giant cell arteritis: a prospective longitudinal study. Medicine. (2016) 95:e3210. doi: 10.1097/MD.0000000000003210
24. Muratore F, Kermani TA, Crowson CS, Green AB, Salvarani C, Matteson EL, et al. Large-vessel giant cell arteritis: a cohort study. Rheumatology. (2015) 54:463–70. doi: 10.1093/rheumatology/keu329
25. Chan CC, Paine M, O’Day J. Steroid management in giant cell arteritis. Br J Ophthalmol. (2001) 85:1061–4. doi: 10.1136/bjo.85.9.1061
26. Hayreh SS, Zimmerman B, Kardon RH. Visual improvement with corticosteroid therapy in giant cell arteritis. Report of a large study and review of literature. Acta Ophthalmol Scand. (2002) 80:355–67. doi: 10.1034/j.1600-0420.2002.800403.x
27. Hayreh SS, Biousse V. Treatment of acute visual loss in giant cell arteritis: should we prescribe high-dose intravenous steroids or just oral steroids? J Neuroophthalmol. (2012) 32:278–87. doi: 10.1097/WNO.0b013e3182688218
28. Rheumatology. Osteoporosis. (2021). Available online at: https://metodebok.no/index.php?action=topic&item=AtEEtJ7q (accessed May 01, 2022).
29. Ponte C, Monti S, Scire CA, Delvino P, Khmelinskii N, Milanesi A, et al. Ultrasound halo sign as a potential monitoring tool for patients with giant cell arteritis: a prospective analysis. Ann Rheum Dis. (2021) 80:1475–82. doi: 10.1136/annrheumdis-2021-220306
30. Seitz L, Christ L, Lotscher F, Scholz G, Sarbu AC, Butikofer L, et al. Quantitative ultrasound to monitor the vascular response to tocilizumab in giant cell arteritis. Rheumatology (Oxford). (2021) 60:5052–9. doi: 10.1093/rheumatology/keab484
31. Kerr GS, Hallahan CW, Giordano J, Leavitt RY, Fauci AS, Rottem M, et al. Takayasu arteritis. Ann Intern Med. (1994) 120:919–29.
32. Jese R, Rotar Z, Tomsic M, Hocevar A. The role of colour doppler ultrasonography of facial and occipital arteries in patients with giant cell arteritis: a prospective study. Eur J Radiol. (2017) 95:9–12. doi: 10.1016/j.ejrad.2017.07.007
33. Chrysidis S, Duftner C, Dejaco C, Schafer VS, Ramiro S, Carrara G, et al. Definitions and reliability assessment of elementary ultrasound lesions in giant cell arteritis: a study from the OMERACT Large Vessel Vasculitis Ultrasound Working Group. RMD Open. (2018) 4:e000598. doi: 10.1136/rmdopen-2017-000598
34. Andel PM, Chrysidis S, Geiger J, Haaversen A, Haugeberg G, Myklebust G, et al. Diagnosing giant cell arteritis: a comprehensive practical guide for the practicing rheumatologist. Rheumatology. (2021) 60:4958–71. doi: 10.1093/rheumatology/keab547
Keywords: giant cell arteritis (GCA), large vessel vasculitis, guidelines, diagnosis, treatment
Citation: Haaversen AB, Brekke LK, Bakland G, Rødevand E, Myklebust G and Diamantopoulos AP (2023) Norwegian society of rheumatology recommendations on diagnosis and treatment of patients with giant cell arteritis. Front. Med. 9:1082604. doi: 10.3389/fmed.2022.1082604
Received: 28 October 2022; Accepted: 12 December 2022;
Published: 06 January 2023.
Edited by:
Ryu Watanabe, Osaka Metropolitan University, JapanReviewed by:
Alojzija Hocevar, University Medical Center Ljubljana, SloveniaHubert De Boysson, Centre Hospitalier Universitaire de Caen, France
Marcin Milchert, Pomeranian Medical University, Poland
Copyright © 2023 Haaversen, Brekke, Bakland, Rødevand, Myklebust and Diamantopoulos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andreas P. Diamantopoulos,  adiamanteas@gmail.com
adiamanteas@gmail.com